

Withdrawal or Relapse? How to Tell the Difference When Stopping Psychiatric Medication
By Dr. Anindo Mitra | MBBS, MD Psychiatry (JIPMER) | Consultant Psychiatrist, Athena Behavioural Health, Gurugram
TL;DR
Withdrawal symptoms and relapse of a psychiatric disorder can look almost identical — anxiety, low mood, insomnia, and agitation appear in both
The key differences are timing, pattern, and the presence of physical symptoms that do not belong to the original diagnosis
Withdrawal typically starts within days of reducing or stopping a medication; relapse builds more slowly
Withdrawal symptoms often improve if the dose is temporarily held or slightly increased; relapse does not
Misidentifying withdrawal as relapse is one of the most common reasons people stay on psychiatric medications longer than necessary
Introduction
There is a moment that happens frequently in psychiatric practice — and it almost certainly happens more often outside of it, in the gap between prescription refills and clinic appointments.
Someone reduces their antidepressant or benzodiazepine, begins to feel worse, and concludes that they cannot stop. The medication goes back up. Sometimes a new prescription is written. And the working assumption, made quickly and often without examination, is that the underlying condition has returned.
That assumption is sometimes correct. But frequently it is not.
What many people experience when reducing or stopping a psychiatric medication is withdrawal — a physiological response to the brain adjusting to the absence of a drug it has adapted to — not the return of the illness the medication was prescribed for. The two can feel almost indistinguishable. Knowing how to tell them apart changes everything about what happens next.
This post lays out the clinical distinctions that matter: for anyone who is currently tapering a medication, anyone who has tried and given up, and anyone whose doctor has never had this conversation with them.
Why This Distinction Is So Difficult
Psychiatric withdrawal symptoms look like psychiatric symptoms. This is not a coincidence — it reflects how these drugs work.
Antidepressants increase serotonin availability at synapses. Over weeks and months of regular use, the brain adapts by reducing its own serotonin receptor density. When the drug is stopped or reduced, serotonin signalling drops — and anxiety, low mood, and poor sleep follow. These are the same symptoms that may have prompted the antidepressant prescription in the first place.
Benzodiazepines work through the GABA system. Long-term use reduces the brain's own GABAergic tone. Withdrawal produces anxiety, hyperarousal, poor sleep, and sometimes physical symptoms — again, a presentation that closely resembles an anxiety disorder.
Horowitz and Taylor, writing in BJPsych Advances (2022), showed that withdrawal symptoms can raise scores on standard depression rating scales — the Hamilton Rating Scale for Depression and the Montgomery-Åsberg Depression Rating Scale — to levels that would formally meet criteria for relapse. This means that even structured clinical assessments can misclassify withdrawal as a return of illness, particularly when no one is looking for withdrawal in the first place.
The stakes of getting this wrong are real. Misdiagnosed withdrawal leads to medication reinstatement, longer treatment duration, and — in some cases — dose escalation. The person who could have come off their medication does not, and may never try again.
The Four Clinical Markers That Help Distinguish Withdrawal From Relapse
These are the criteria used in clinical practice, drawn from the work of Horowitz and Taylor (BJPsych Advances, 2022) and NICE. No single marker is definitive — the picture as a whole is what matters.
1. Timing of Onset
Withdrawal symptoms begin soon after a dose reduction — typically within 2–4 days for short-acting drugs (paroxetine, alprazolam, venlafaxine) and within 1–2 weeks for longer-acting ones (fluoxetine, clonazepam). The closer the symptom onset is to the dose change, the more likely it reflects withdrawal.
Relapse of depression or an anxiety disorder builds more gradually. A genuine recurrence of depression typically takes weeks to months to emerge after stopping a medication — it does not usually arrive within three days of a dose reduction.
This timing distinction is the single most useful clinical marker. If someone feels significantly worse within a week of reducing their medication, the working hypothesis should be withdrawal until proven otherwise.
2. The Presence of Physical Symptoms
This is the marker that gets missed most often.
Withdrawal from antidepressants and benzodiazepines produces physical symptoms that do not belong to the original psychiatric diagnosis:
Brain zaps — brief electrical-shock sensations in the head, often triggered by eye movement. These are almost pathognomonic of antidepressant discontinuation and have no equivalent in relapse of depression or anxiety.
Dizziness and vertigo — one of the most commonly reported discontinuation symptoms. A 2025 systematic review and meta-analysis found dizziness was associated with a five-fold increase in odds during antidepressant discontinuation compared to placebo.
Nausea and gastrointestinal disturbance
Flu-like symptoms — aching muscles, chills, fatigue in the absence of infection
Sweating, especially nocturnal
Tremor and electric-shock sensations in the limbs
Depression does not cause brain zaps. Generalised anxiety disorder does not cause vertigo and nausea in the absence of panic. When these symptoms appear in the context of a dose reduction, they are almost certainly withdrawal.
The reverse is also useful clinically. If someone stops a medication and feels worse but has no physical symptoms at all — just a return of familiar, previously experienced depressive or anxious feelings, building gradually over weeks — relapse becomes more likely.
3. Response to Reinstatement
Withdrawal symptoms typically resolve quickly — often within 24–48 hours — when the medication is reinstated or the dose returned to the previous level. NICE notes this rapid reversal as characteristic of withdrawal: prompt symptom resolution when the dose is reinstated strongly suggests those symptoms were caused by its absence.
Relapse does not respond this quickly. A genuine depressive episode does not remit within two days of restarting an antidepressant — antidepressants take weeks to achieve their effect. Rapid symptom resolution with reinstatement is withdrawal. Slow, gradual improvement over weeks is more consistent with a medication working on relapsed illness.
One important caveat: if reinstatement is delayed by several weeks, the response becomes less predictable. The window for rapid resolution of withdrawal symptoms through reinstatement is relatively narrow.
4. Pattern Over Time — the Wave
Withdrawal symptoms do not follow a linear course. They often come in waves — periods of feeling quite bad, followed by brief windows of improvement, then another wave. This undulating pattern is characteristic of withdrawal and different from the more sustained, persistent low that typifies a depressive relapse.
At each dose reduction step during a taper, symptoms may worsen transiently, then settle. This is the expected pattern. Recognising it prevents patients from concluding that they need to stop the taper — they often just need to hold at the current dose until the wave passes.
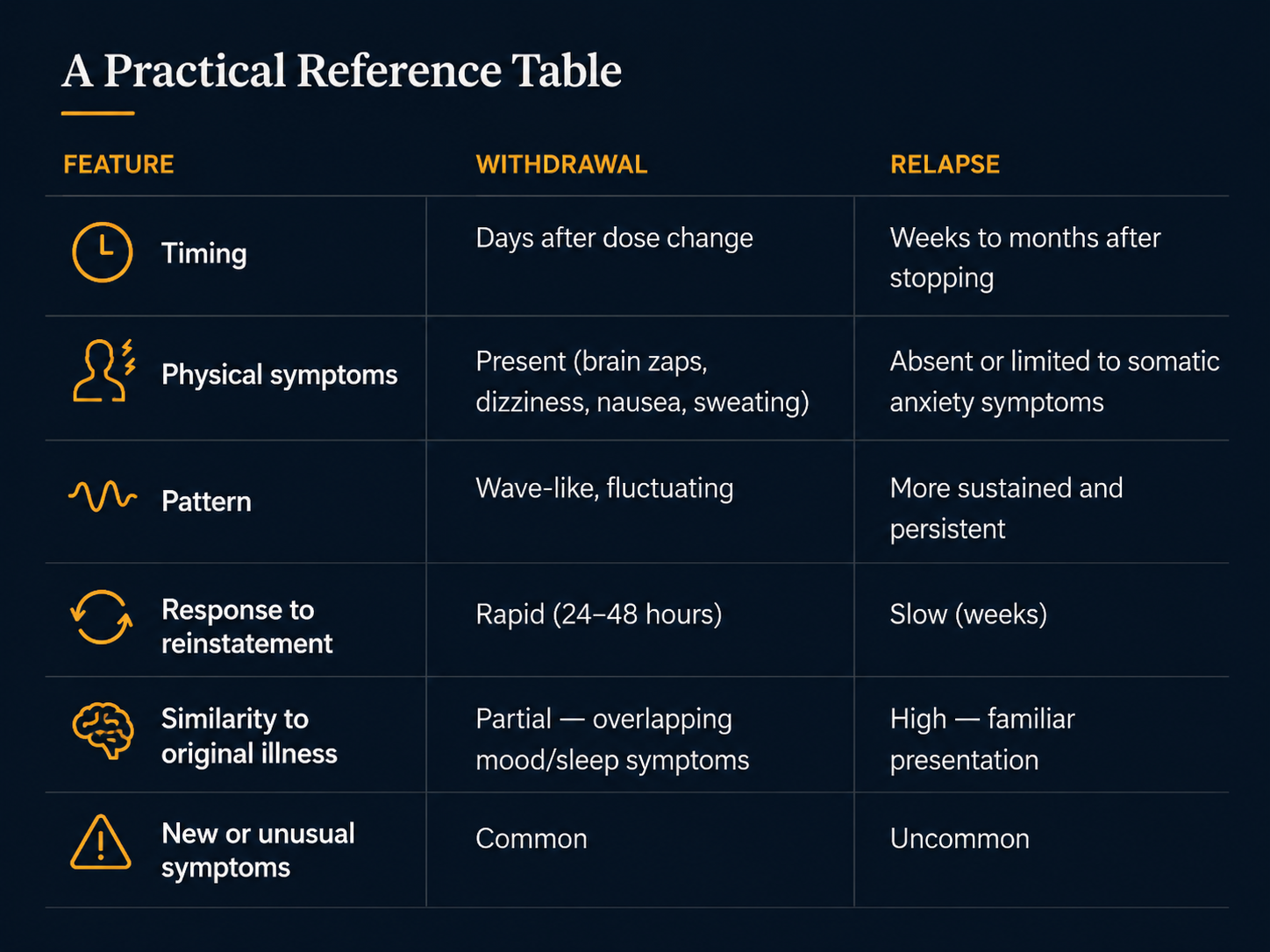
Withdrawal vs Relapse
How Common Is This Problem?
The scale of antidepressant discontinuation symptoms is often underestimated. 2024 systematic review and meta-analysis in The Lancet Psychiatry found that, accounting for placebo effects, approximately 15% of patients experience discontinuation symptoms when stopping antidepressants — equivalent to roughly 1 in 6 or 7 people. For paroxetine and venlafaxine, rates in older studies ran higher: 60–66% in a US trial examining discontinuation over 5–8 days.
These numbers likely undercount the problem. Most discontinuation studies use abrupt or rapid cessation rather than gradual tapering, which inflates withdrawal rates and makes them harder to distinguish from relapse. Studies rarely use validated withdrawal-specific scales. And the research has historically been more focused on whether the drug prevents relapse than on what stopping it actually feels like.
For benzodiazepines, the picture is similar. An internet survey of 1,207 psychiatrists in the US (2018–2019) documented a syndrome of protracted withdrawal symptoms — lasting months or years after stopping — that had not been adequately characterised in the formal literature. This protracted withdrawal is worth knowing about because it can be misidentified as a new psychiatric disorder, prompting further medication rather than continued support through the withdrawal process.
The Specific Problem With Antidepressants: When Withdrawal Looks Like Relapse in Trials
There is a subtler dimension to this that matters clinically and is worth understanding.
Much of what we know about whether antidepressants prevent relapse comes from discontinuation studies — trials where patients who are well on antidepressants are randomly assigned to continue the drug or switch to placebo. Those who switch to placebo and deteriorate are counted as having relapsed, which is used as evidence that the drug is preventing future episodes.
Horowitz and Taylor (BJPsych Advances, 2022) argue compellingly that a proportion of what these studies call "relapse" is actually withdrawal — particularly because discontinuation in these trials is typically abrupt or rapid, which maximises the chance of withdrawal symptoms. If this is correct, the evidence base for long-term antidepressant use in depression prevention may be less robust than currently assumed.
This is not a settled question. But for clinicians managing patients who want to stop antidepressants, it reinforces the importance of slow tapering, careful symptom monitoring, and applying the clinical markers above before concluding that a worsening represents relapse.
What to Do If You Are Not Sure
In practice, uncertainty is common. Withdrawal and relapse can coexist — particularly if the underlying condition was not fully treated before the medication was started. The following approach is reasonable when the picture is unclear:
Hold, don't restart. If symptoms emerge after a dose reduction, hold at the current dose and wait 2–4 weeks before concluding anything. Many withdrawal symptoms settle at a held dose without needing to go back up.
Look for the physical markers. Brain zaps, dizziness, nausea, and flu-like symptoms strongly favour withdrawal. Their absence does not rule out withdrawal, but their presence should shift the working hypothesis firmly toward it.
Consider a small increase, not a full return. If symptoms are severe, reinstating a fraction of the reduction (not the full original dose) can relieve withdrawal while maintaining some progress. This should be done with clinical supervision.
Track the timing. Keep a simple daily note of symptom severity and when dose changes were made. This creates the temporal data needed to make the distinction.
Speak with your psychiatrist before concluding you need to stay on the medication permanently. The distinction between withdrawal and relapse should be made collaboratively, with awareness of all the clinical markers above, not assumed by default.
Conclusion
Withdrawal from psychiatric medication and relapse of a psychiatric disorder are genuinely different things. They can look similar because they share neurobiology. But the timing, the physical symptoms, the response to reinstatement, and the pattern over time give enough clinical information to distinguish one from the other in most cases.
The reason this matters is not academic. Misclassifying withdrawal as relapse keeps people on medications they could potentially stop. A systematic application of these clinical markers — by psychiatrists and by informed patients — is one of the most practical tools in rational deprescribing.
If you are currently trying to come off a psychiatric medication and finding it harder than expected, it is worth having this conversation with your treating clinician explicitly. The question "Is this withdrawal or relapse?" should be part of every deprescribing plan. If it has not come up, bring it up.
Explore More in This Series
This post is part of the Deprescribing series on dranindomitra.com:
Am I Ready to Stop My Antidepressant? A Psychiatrist's Checklist (coming soon)
Are Psychiatric Medications Addictive? The Honest Answer (coming soon)
How Long Should You Actually Be on a Psychiatric Medication? (coming soon)
Or visit the Deprescribing overview page for the full picture.
Dr. Anindo Mitra is a Consultant Psychiatrist at Athena Behavioural Health, Gurugram. He completed his MD in Psychiatry from JIPMER, Puducherry. His clinical interests include rational psychopharmacology, deprescribing, and the long-term management of anxiety and mood disorders.
This post is for educational purposes only. It does not constitute individualised medical advice. If you are considering stopping any psychiatric medication, please consult your treating psychiatrist.
FAQ
Q: How quickly do withdrawal symptoms appear after stopping an antidepressant?
It depends on the specific drug. For short-acting antidepressants like paroxetine or venlafaxine, symptoms can begin within 1–3 days. For longer-acting ones like fluoxetine, onset may be delayed by a week or more. Symptoms appearing within a few days of stopping or reducing a dose should be assumed to be withdrawal unless there is clear reason to think otherwise.
Q: Can withdrawal symptoms last for months?
Yes, though this is more common after long-term use at higher doses. A small proportion of people experience protracted withdrawal — low-level symptoms persisting for months after the last dose. This is not permanent brain damage; most people recover fully. Ongoing psychiatric and psychological support during this period is important, as is ensuring that these symptoms are not misidentified as new psychiatric illness.
Q: If my depression came back after stopping my antidepressant, does that mean I need to be on it forever?
Not necessarily. The first step is determining whether what appeared to be relapse was actually withdrawal. If true relapse has occurred — confirmed by its slower onset, absence of physical symptoms, and non-response to reinstatement within days — then a longer treatment course may be appropriate. But this decision should be made explicitly, with an agreed future plan for a supervised taper, not by default.
Q: Are some antidepressants more likely to cause withdrawal?
Yes. Paroxetine and venlafaxine are consistently associated with higher rates of discontinuation symptoms than other antidepressants, largely because of their short half-lives and potent serotonergic effects. Fluoxetine, with its very long half-life, is associated with significantly lower rates. This pharmacological difference is relevant to both choice of initial antidepressant and to switching strategies during a taper.
Q: Is there a test that can confirm whether what I'm experiencing is withdrawal or relapse?
There is no blood test or scan. The distinction is clinical, based on timing, symptom pattern, physical markers, and response to dose change. This is why careful clinical documentation — keeping a symptom diary with dates of dose changes — is so practically useful. It creates the evidence needed to make the distinction.
Q: Does the same withdrawal-vs-relapse logic apply to benzodiazepines?
Yes, though with some differences. Benzodiazepine withdrawal has a more prominent physical component and a greater safety risk (including seizure risk) than antidepressant withdrawal. The timing markers are similar — symptoms appearing within days of dose reduction favour withdrawal — but the physical signs (tremor, sweating, palpitations, depersonalisation) are often more pronounced. Anxiety returning weeks after a benzodiazepine taper without physical symptoms may warrant genuine assessment for whether the underlying anxiety disorder needs separate treatment.